Chronic Atopic Dermatitis With Psoriasiform Spongiotic Features: A 20-Month Steroid-Free Clinical Course Under TCM Herbal Therapy
What Chronic Eczema Recovery Really Looks Like: A 20-Month Documented Case
A single case of chronic atopic dermatitis with psoriasiform spongiotic features, documented over 20 months during herbal TCM treatment.
This is one patient’s story, followed with photographs over nearly two years. It is shared to help patients understand what recovery from long-standing eczema can realistically look like: usually waves, not a straight line.
Case Summary
A 30-year-old Asian male presented with a one-year history of recurrent itchy rashes, most prominently affecting the neck region, with additional involvement of the trunk and legs. He had no known family history of atopic disease and was otherwise healthy.
Before attending our clinic, he had been treated in primary care with topical corticosteroid creams. The rash improved while the steroid cream was being applied, but repeatedly rebounded after discontinuation. Over approximately 10 months, he used about 10 tubes of topical steroid cream, each 15 g.
He subsequently sought dermatological opinion and was prescribed topical antifungal cream together with oral miconazole. After two months of antifungal treatment, the eruption remained persistent and showed little meaningful improvement. He then sought alternative herbal medicine care at our clinic.
Clinical Presentation at First Visit
On examination, the patient presented with chronic itchy dermatitis affecting the neck, upper chest, trunk, and legs. The involved skin appeared reddish, irritated, and inflamed. Some areas, particularly around the neck, showed thickened and leathery texture consistent with long-standing scratching and rubbing.
Small scratch marks and tiny scabs were visible, especially over the neck and upper chest, indicating an ongoing itch–scratch cycle. The neck region was the most severely affected area, likely because skin folds, heat, sweat, and friction from clothing can make this site especially prone to irritation.
Overall, the pattern was more consistent with a chronic eczema-type inflammatory condition than with a new or sudden skin problem.
Investigations and Diagnostic Impression
A skin biopsy was performed from the left chest wall. Blood chemistry, liver function, and kidney function investigations were also ordered.
The biopsy report showed psoriasiform spongiotic dermatitis. Serum IgE was elevated at 226 IU/mL, with a reference range of less than 100 IU/mL. Liver function, renal profile, urinalysis, and the erythrocyte sedimentation rate (ESR 3 mm/hr) were within normal limits, with no laboratory safety concerns identified during the documented course.
Taken together, the clinical picture, chronic itch, relapsing pattern, elevated IgE, and biopsy findings were most consistent with atopic dermatitis as the primary diagnosis, with overlapping psoriasiform and spongiotic histological features.
This mixed pattern may reflect chronic or lichenified atopic dermatitis. It may also suggest a broader inflammatory phenotype involving both type 2 and type 17 immune pathways, which has been described in recent dermatopathology literature.
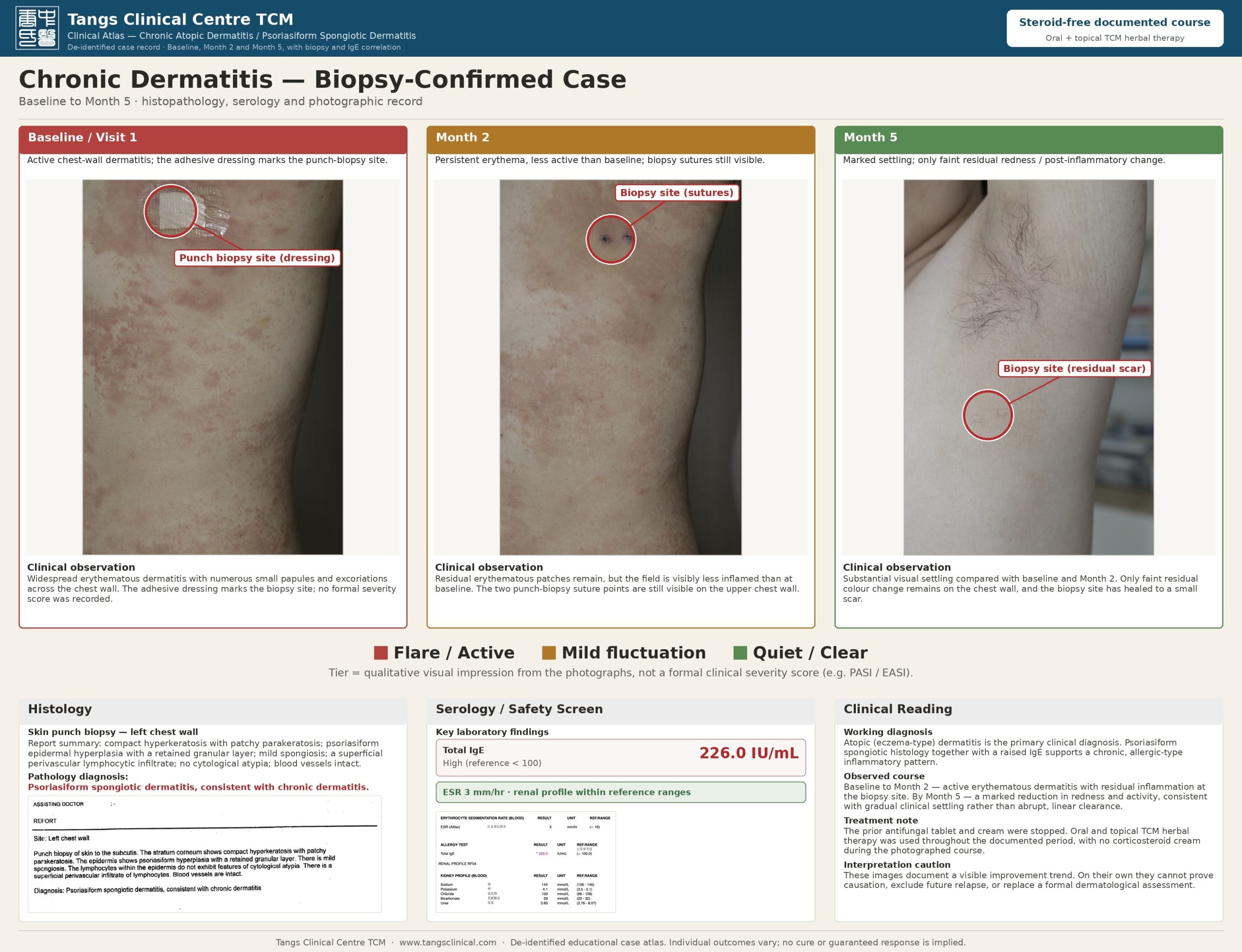
Figure 1. Baseline to Month 5 clinical atlas showing biopsy-site localisation, histology, serum IgE, and photographic progression. The biopsy was taken from the left chest wall at baseline. This atlas documents the chest-wall biopsy region over the first five months; the neck region is documented separately over the full 20 months in Figure 2 (same patient). Image interpretation remains observational and should not replace formal dermatological assessment.
Treatment Course and Photographic Progression
After review, the antifungal tablet and antifungal cream were discontinued. The patient then commenced oral and topical TCM herbal therapy. No corticosteroid cream was used during the documented treatment course.
The photographic series records the patient’s skin changes from baseline to Month 20. Rather than showing a simple straight-line recovery, the clinical course followed a wave-like pattern: periods of improvement were followed by mild fluctuations, but the overall direction was progressively favourable.
- Baseline – Month 2 The most active stage. The neck and upper chest showed patchy redness, oozing, crusting, and visible scratch marks.
- From Month 3 The first marked improvement became visible, with substantial reduction in the extent of inflammation, redness, and swelling.
- Months 4 – 12 A relatively stable but still fluctuating phase, with mild scattered flares around Months 4, 6–8, 11, and 12.
- Month 13 A more distinct relapse, with renewed patchy erythema and scratch marks over the upper chest — clearly milder than the baseline presentation.
- Months 14 – 17 The skin settled again, with further mild fluctuations around Months 16 and 17.
- Month 18 A second more distinct relapse, again milder and shorter than baseline.
- Months 19 – 20 The rash largely settled. By Month 20, the skin appeared more even in colour, with no obvious active dermatitis visible in the documented area.
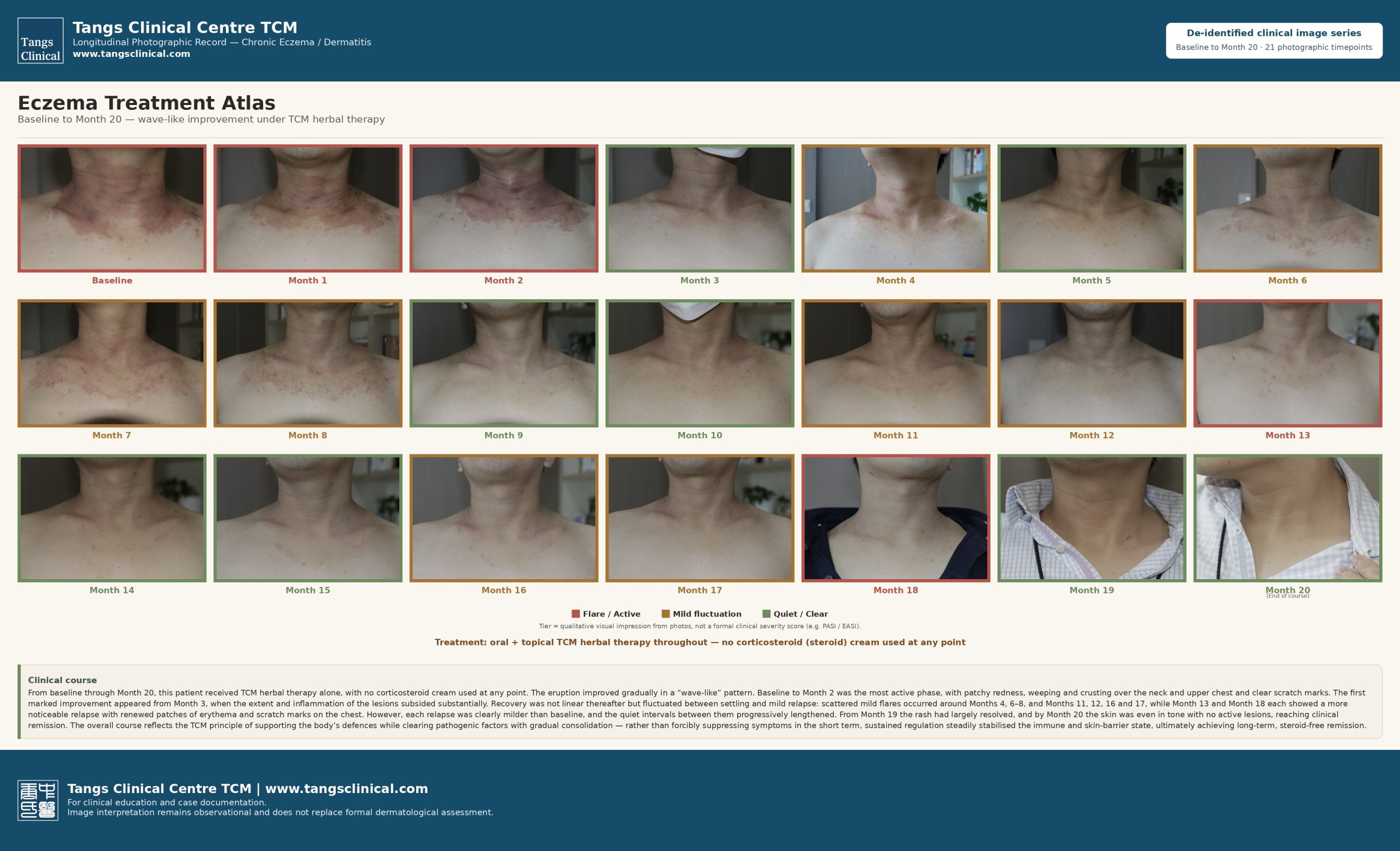 Figure 2. Longitudinal photographic progression of the neck / upper chest from baseline to Month 20. The eruption improved overall in a wave-like and progressive pattern. Baseline to Month 2 represented the most active stage. Scattered mild flares occurred around Months 4, 6–8, 11, 12, 16, and 17, while Months 13 and 18 each showed a more noticeable relapse. From Month 19 onward, the rash had largely settled, and by Month 20 no active lesions were visible in the photographed area. The colour tiers reflect a qualitative visual impression from the photographs, not a formal severity score. Figures 1 and 2 document the same patient at two body sites (chest-wall biopsy region and neck) over different windows.
Figure 2. Longitudinal photographic progression of the neck / upper chest from baseline to Month 20. The eruption improved overall in a wave-like and progressive pattern. Baseline to Month 2 represented the most active stage. Scattered mild flares occurred around Months 4, 6–8, 11, 12, 16, and 17, while Months 13 and 18 each showed a more noticeable relapse. From Month 19 onward, the rash had largely settled, and by Month 20 no active lesions were visible in the photographed area. The colour tiers reflect a qualitative visual impression from the photographs, not a formal severity score. Figures 1 and 2 document the same patient at two body sites (chest-wall biopsy region and neck) over different windows.Recovery Came in Waves, Not a Straight Line
The important clinical lesson from this case is that chronic eczema recovery may not be linear. Patients often expect the rash to disappear quickly and permanently once treatment begins. In reality, especially in long-standing dermatitis, improvement may occur through a sequence of reduced inflammation, shorter flares, longer quiet intervals, and gradual stabilisation of the skin barrier.
In this case, each recurrence was visibly less severe than the baseline presentation, and the stable intervals between flares gradually became longer. This 20-month photographic record is valuable because it shows a credible middle phase: not an instant “before and after,” but a real-world course of fluctuation, relapse, and consolidation before clinical remission.
Discussion
This case illustrates a chronic relapsing dermatitis with both clinical and histological features overlapping eczema and psoriasiform dermatitis.
Elevated IgE is commonly associated with type 2 inflammation and supports the diagnosis of atopic dermatitis. Classic atopic dermatitis usually demonstrates spongiotic features on histology, but chronic scratching and lichenification may produce psoriasiform epidermal thickening. This can create a mixed biopsy pattern described as psoriasiform spongiotic dermatitis.
Recent studies have suggested that some cases of spongiotic psoriasiform dermatitis may represent a hybrid inflammatory phenotype, with co-activation of both Th2 and Th17 immune pathways. This may partly explain why certain patients respond incompletely to conventional single-axis treatments.
In this patient, the clinical pattern strongly supported chronic atopic dermatitis: persistent itch, relapsing-remitting behaviour, involvement of friction-prone areas such as the neck, elevated IgE, and biopsy evidence of spongiotic dermatitis. The psoriasiform component may reflect chronicity and repeated scratching, although a mixed inflammatory phenotype remains a reasonable consideration.
Clinical Takeaways for Patients
- Chronic eczema often behaves in waves rather than as a straight-line recovery.
- Rebound after stopping steroid cream may occur, especially when underlying inflammation and skin-barrier weakness remain unresolved.
- Visible improvement can begin early, but deeper stabilisation may require longer-term monitoring and consistent care.
- A temporary flare during treatment does not always mean treatment failure. The severity, duration, and frequency of each flare should be compared with the original baseline.
- In this case, later flares were milder, shorter, and separated by longer quiet intervals before the skin reached clinical remission in the photographed area.
Frequently Asked Questions
Can Traditional Chinese Medicine cure eczema?
No treatment — conventional or traditional — should be described as “curing” eczema, because eczema is usually a chronic, relapsing condition. This single case showed improvement during TCM herbal treatment, but one patient’s experience cannot prove causation or guarantee the same result for others.
Why does eczema come back after stopping steroid cream?
Steroid creams reduce visible inflammation, but they do not remove the underlying inflammatory tendency or fully repair a weakened skin barrier. When the cream is stopped, the rash may return. In some patients, especially after frequent or prolonged use, rebound flaring can be more noticeable. Medication changes should be discussed with the prescribing doctor.
Does a flare during treatment mean treatment has failed?
Not necessarily. A single flare does not automatically mean treatment failure. What matters more is the trend over time: whether flares are becoming milder, shorter, and further apart compared with the original baseline.
How long does chronic eczema recovery take?
It varies widely. In this case, clear improvement was visible from around Month 3, but the skin continued to fluctuate for many months before settling more consistently around Months 19–20. This is one person’s course, not a guaranteed timeline.
Professional Commentary and Methodological Notes
Clinicopathologic Correlation
This case supports the importance of clinicopathologic correlation in chronic dermatitis. A biopsy diagnosis of psoriasiform spongiotic dermatitis should not be interpreted in isolation. The final working diagnosis depends on the integration of morphology, distribution, itch pattern, laboratory findings such as IgE, histopathology, and treatment response.
Diagnostic Interpretation
Where clinical features favour atopic dermatitis and IgE is elevated, psoriasiform changes may represent chronic lichenification. However, if clinical ambiguity persists or treatment response is poor, clinicians may consider a broader mixed inflammatory phenotype involving both Th2 and Th17 pathways.
Topical Steroid Withdrawal Consideration
Prolonged corticosteroid use (approximately 10 months) on thin, friction-prone skin, with relapse on each discontinuation, is compatible with a rebound / topical steroid withdrawal component. Because steroids were stopped at intake, part of the early improvement may reflect post-steroid recovery rather than a treatment effect alone. This differential is retained and limits any causal interpretation.
TCM Perspective
From a TCM perspective, the course is consistent with gradual regulation rather than short-term suppression: active inflammation settled first, repeated flares became progressively milder, and the skin barrier appeared more stable over time. The traditional principle may be described as “supporting the body’s defences while clearing pathogenic factors, with gradual consolidation.” This is a therapeutic-reasoning framework, not a demonstrated biological mechanism.
Limitations
- This is a single case and cannot establish causality.
- Atopic dermatitis naturally waxes and wanes; a topical steroid withdrawal component cannot be excluded, so improvement cannot be attributed to the herbal therapy alone.
- No validated severity score (e.g. EASI, SCORAD, IGA) was applied; tiers are a qualitative visual impression.
- Lighting, distance, camera angle, and exposure may affect photographic comparison.
- Outcome interpretation remains observational.
- This article does not replace formal dermatological diagnosis or treatment planning.
Ethics and Consent
The patient provided written informed consent for the use of de-identified clinical photographs and case details for educational and clinical-discussion purposes. Identifying information has been removed, and no full name, exact date of birth, contact details, identification number, or identifiable facial image is included.



