Systemic Regulation and Homeostatic Reconstruction in Chronic Atopic Dermatitis: A 70-Month Clinical Follow-up Analysis of a Patient with a 37-Year Medical History 慢性特应性皮炎的系统性调节与稳态重建:一例37年病史患者的70个月临床随访分析
Summary
A 70-month (nearly 6-year) longitudinal documentation of comprehensive skin restoration. This report details the journey of a female patient with a 37-year history of severe Chronic Eczema (Atopic Dermatitis). After discontinuing decades of corticosteroid dependency, she achieved complete “dermal remodeling” and clinical remission through a staged, individualized herbal systemic regulation protocol. We aren’t just suppressing symptoms; we are spending six years to reprogram thirty-seven years of inflammatory memory.
Core Clinical Observations:
- Non-linear Recovery Trajectory: The path to healing was not instantaneous but evolved through four distinct physiological milestones: an initial “Inflammatory Surge” (Topical Steroid Withdrawal phase), followed by “Immune Correction,” “Structural Remodeling,” and finally, the establishment of “Long-term Homeostasis.”
- Breaking the Suppression-Rebound Cycle: Traditional “suppression-rebound” symptomatic treatments often fail to address the root of chronic inflammation. This case demonstrates that Systemic Immune Regulation can effectively reconstruct the compromised skin barrier and quell overactive “immune memory” at the cellular level.
- The Intersection of Biological Time and Clinical Value: Repairing an immune system conditioned by over 30 years of pathology requires a “biological timescale” proportionate to its depth. Over the 70-month follow-up period, the patient achieved sustained, drug-free clinical remission—offering a new paradigm and robust scientific evidence for the long-term management of refractory Atopic Dermatitis.
———————————————-
Chronic Eczema (Atopic Dermatitis, AD) is a complex chronic inflammatory skin disease characterized by significant immune dysregulation, disruption of the skin barrier, and intense pruritus. Epidemiological data indicate that in some patients, the condition begins in childhood and persists into adulthood or even throughout life. Traditional treatment has primarily relied on topical corticosteroids, often resulting in a “control → rebound → worsening” cycle, posing substantial challenges for both patients and clinical management [1-5].
Case Background
A 37-year-old female patient had a history of eczema since infancy, with a cumulative disease duration of 37 years. Under conventional management, she had long-term use of topical corticosteroids. Although symptoms were temporarily relieved, they rapidly recurred upon discontinuation, with each relapse becoming more severe. This repeated inflammatory cycle failed to fundamentally stabilize the immune system and instead deepened chronic structural skin changes and itch sensitivity.
The patient did not receive modern biologic therapy. Instead, she underwent individualized herbal (botanical) treatment at Tangs Clinical TCM, with monthly follow-ups and dynamic formula adjustments. She was continuously monitored for 70 months (approximately six years). Through staged photographic documentation and clinical evaluation, long-term changes in skin condition were observed.
Milestone Analysis of Clinical Recovery
Over six years of treatment, the patient’s skin evolved from an “active inflammatory state” to “structural repair” and finally to “homeostatic maintenance.” This gradual and steady improvement reflects the true remodeling trajectory of chronic eczema: inflammation resolves before thickness improves, and restoration of skin thickness and neural sensitivity often requires a longer period [6-8].
Initial Phase (Months 0–9): Concentrated Release of Inflammatory Burden

During the first few months after complete discontinuation of corticosteroids, the patient exhibited persistent erythema and marked lichenification, consistent with a typical Topical Steroid Withdrawal (TSW) response. Skin inflammation significantly worsened, with increased erythema, pruritus, and hypersensitivity, reflecting local immune dysregulation and rebound immune activation [9-12]. The skin was extremely fragile during this period. Clinical management focused on systemic regulation to mitigate acute inflammatory peaks.
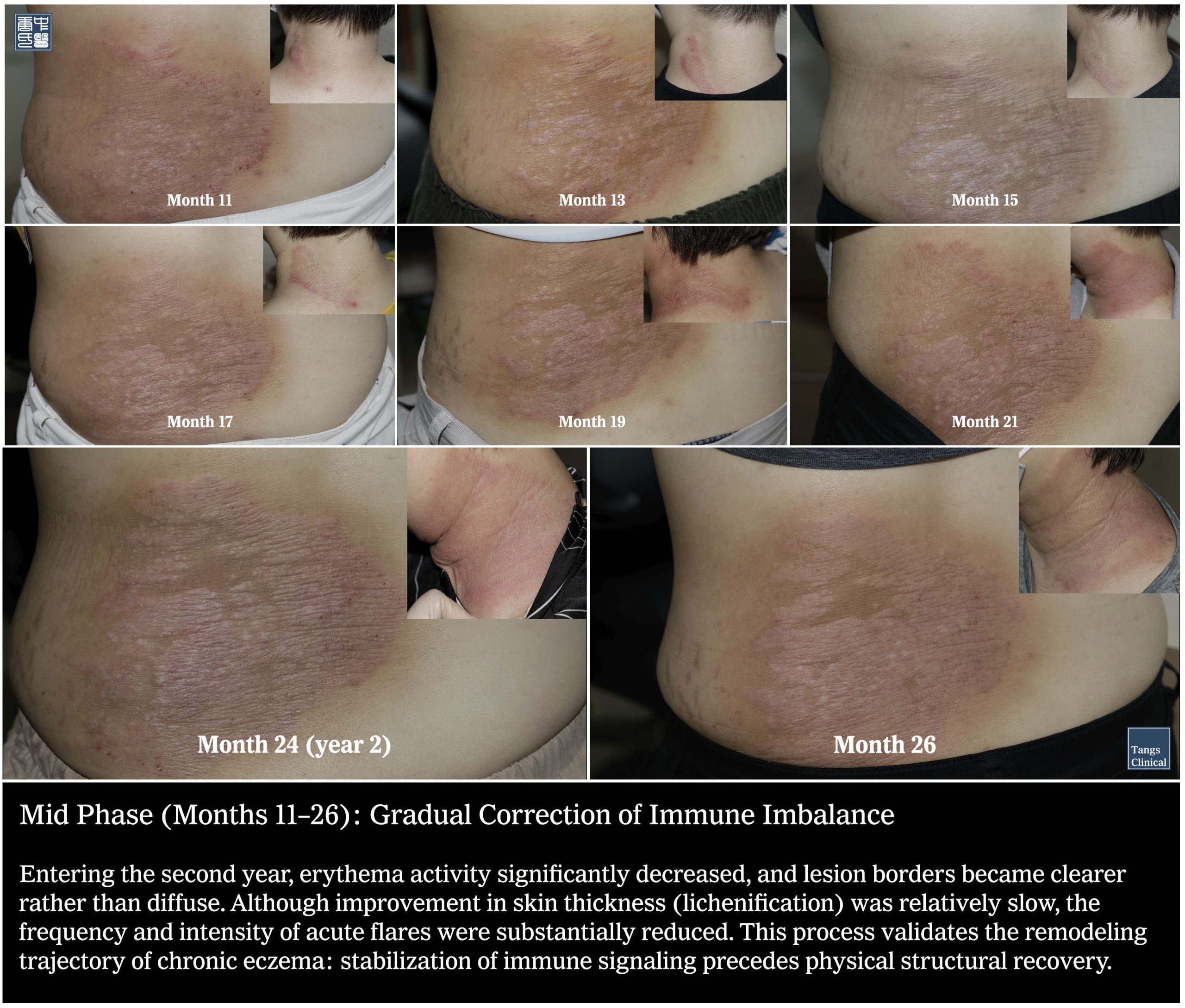
Mid Phase (Months 10–26): Gradual Correction of Immune Imbalance
atopic-dermatitis-70-month-recovery-tcm
Entering the second year, erythema activity significantly decreased, and lesion borders became clearer rather than diffuse. Although improvement in skin thickness (lichenification) was relatively slow, the frequency and intensity of acute flares were substantially reduced. This process validates the remodeling trajectory of chronic eczema: stabilization of immune signaling precedes physical structural recovery.
Late Phase (Months 28–46): Substantial Epidermal Structural Remodeling
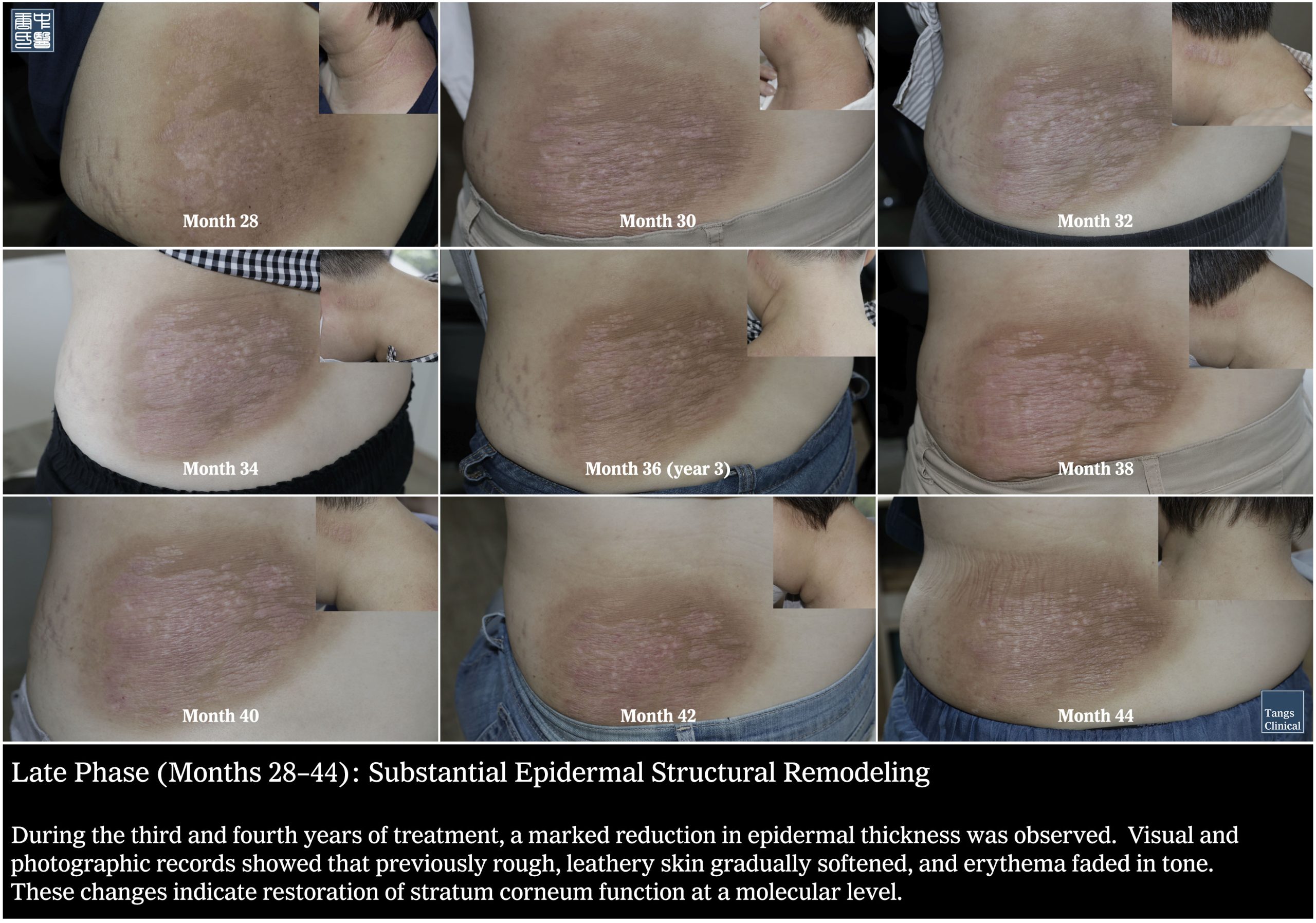
During the third and fourth years of treatment, a marked reduction in epidermal thickness was observed. Visual and photographic records showed that previously rough, leathery skin gradually softened, and erythema faded in tone. These changes indicate restoration of stratum corneum function at a molecular level.
Stable Phase (Months 48–70): Establishment of Long-Term Homeostasis
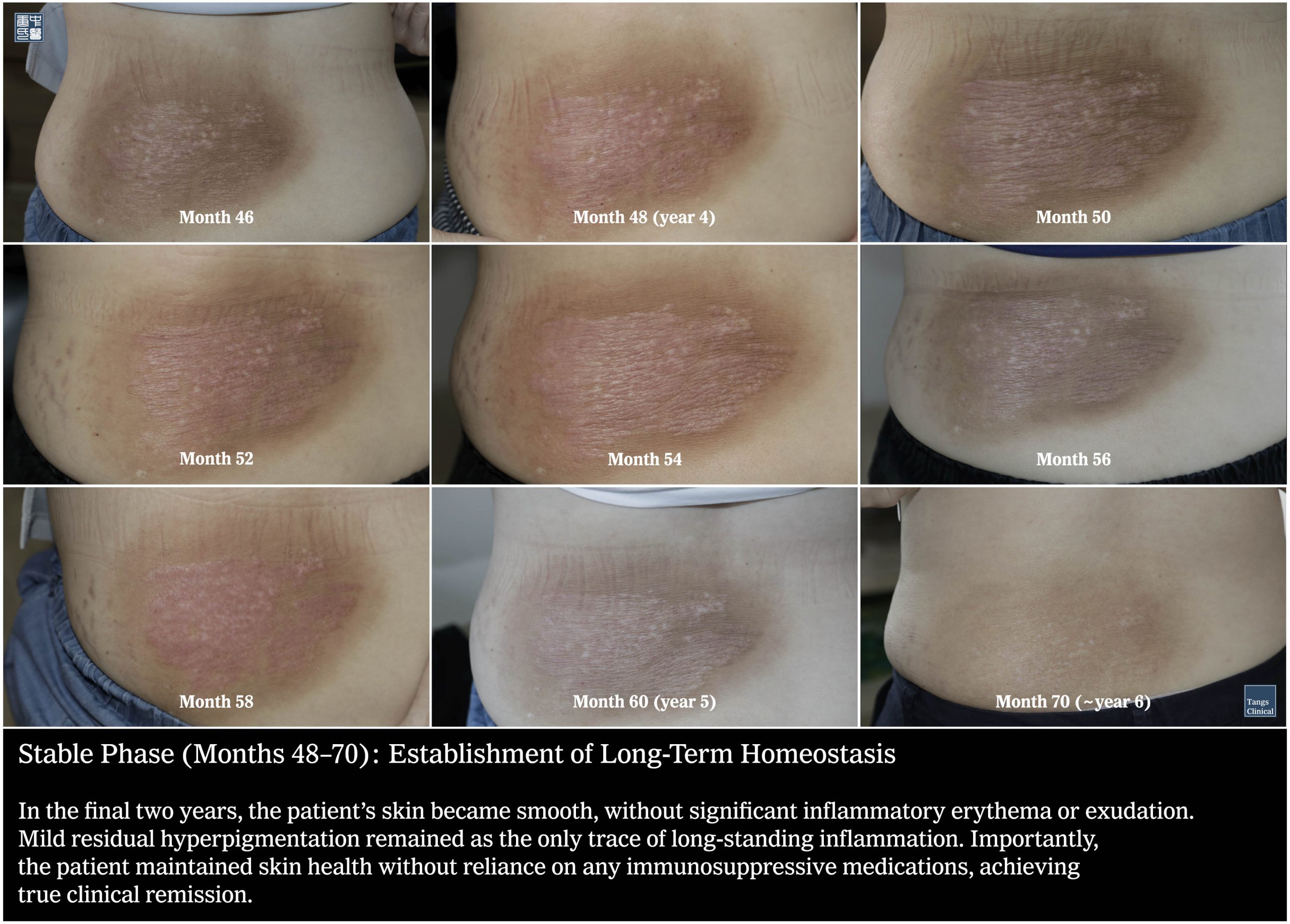
In the final two years, the patient’s skin became smooth, without significant inflammatory erythema or exudation. Mild residual hyperpigmentation remained as the only trace of long-standing inflammation. Importantly, the patient maintained skin health without reliance on any immunosuppressive medications, achieving true clinical remission.
Major Determinant: History of Repeated Corticosteroid Use
Extensive clinical experience and academic literature suggest that repeated use of topical corticosteroids not only fails to cure chronic eczema but may lead to Topical Steroid Withdrawal (TSW), characterized by intensified erythema, pruritus, and heightened skin sensitivity after cessation [9-12].
The prolonged cycle of “suppression → rebound → re-suppression” causes continuous fluctuation in immune status and skin structure, thereby deepening chronic pathological changes. Literature indicates that the longer corticosteroids are used, the longer it takes to return to immune homeostasis—an observation directly reflected in this case [10,13-17].
Scientific Basis of Systemic Regulation
The treatment in this case was not simply anti-inflammatory suppression. Rather, through syndrome differentiation and individualized herbal prescriptions, systemic regulation was applied to gradually correct immune imbalance and barrier dysfunction, aligning with modern chronic disease management concepts:
- Immune modulation at a systemic level: Experimental studies have shown that active components in certain herbal formulas can regulate inflammatory cytokines (such as IL-4 and IL-13), promote Th1/Th2 balance, and reduce allergic response intensity [18-25].
- Enhancement of barrier function: Some botanical extracts can increase the expression of key structural proteins in the stratum corneum (such as filaggrin and ceramide synthesis pathways), helping restore the natural skin barrier [26-29].
- Regulation of neuro-immune interaction: Chronic pruritus partly stems from neural sensitization. Systemic herbal regulation may buffer this sensitivity, reduce scratching behavior, and improve sleep quality [30-36].
These mechanisms align with current systemic management approaches to chronic inflammation. Rather than simply suppressing inflammation, this strategy emphasizes restoring overall homeostasis across immune, barrier, and neural dimensions.
Literature Support and Scientific Foundation
Numerous studies have demonstrated the central roles of immune modulation and barrier repair in chronic eczema:
- Modern pathophysiological analyses suggest that chronic eczema involves not only local inflammation but also immune memory and systemic inflammatory baseline reprogramming [1,37-39].
- Review studies indicate that certain herbal components possess anti-inflammatory, antioxidant, and barrier-supportive properties and have been incorporated into traditional medical systems for chronic inflammatory states [40-49].
- Clinical research on the recurrent nature of chronic eczema suggests that suppressing inflammatory signals alone does not guarantee long-term stability; higher-level immune homeostasis must be restored. Molecular profiling and transcriptomic studies show that even after visible inflammation resolves, subclinical immune activation persists in clinically normal skin, including ongoing dysregulation of Th1, Th2, and Th17 pathways, chemokine signaling, and barrier dysfunction. This persistent subclinical inflammation is a key driver of disease relapse and recurrence, indicating that targeting only acute inflammatory signals is insufficient for durable remission. Longitudinal studies confirm that proactive maintenance therapy and strategies aimed at correcting subclinical inflammation and restoring immune homeostasis reduce relapse rates and improve long-term outcomes, compared to approaches that focus solely on suppressing visible inflammation. Furthermore, immune memory and skin-homing T cells play a central role in recurrent episodes, underscoring the need for therapies that address systemic and local immune reprogramming rather than just acute suppression. Clinical trials of targeted biologics (e.g., IL-4/IL-13 blockade) show that while these agents can suppress type 2 inflammation and improve symptoms, a significant proportion of patients do not achieve complete or sustained remission, highlighting the importance of restoring broader immune balance and barrier function for long-term disease control [1,50-54].
These literature foundations are consistent with the long-term follow-up findings in this case, indicating that systemic adjustment of chronic pathology requires a longer biological time scale rather than short-term suppression.
Clinical and Scientific Implications
- Long-Term Management ≠ Delayed Healing
The reconstruction process in chronic eczema is fundamentally a rebuilding of immune–structural–neural homeostasis. Its time scale should correspond to the depth of pathology. - Corticosteroid History as a Key Weighting Factor
Long-term repeated use of topical corticosteroids is a major modifiable factor influencing treatment resistance and prolonged recovery. - Systemic Advantage of Individualized Herbal Regulation
Compared with purely suppressive symptom-based strategies, this approach focuses on comprehensive immune and barrier reconstruction, aligning with modern chronic disease management principles.
Conclusion
In a clinical case of chronic eczema lasting over 30 years, individualized herbal compound therapy combined with continuous monthly follow-ups ultimately achieved progressive inflammatory control, structural tissue improvement, and long-term stability. This trajectory reflects the authentic process of homeostatic reconstruction in chronic inflammatory disease.
Similar to the concept of precision medicine in modern healthcare, individualized herbal regulation emphasizes dynamic adjustment of formulations according to the patient’s real-time condition (syndrome differentiation), functioning essentially as a highly flexible feedback system.
Key Takeaways
- The duration of treatment is not the sole measure of efficacy. Instead, it reflects a biological time scale closely related to pathological depth, historical treatment patterns, and immune and barrier status.
- The greatest challenge this report poses to the medical field is the redefinition of “efficacy.” If evaluated over one month, the treatment might be judged as slow-acting; if evaluated over ten years, its drug-free homeostasis offers exceptionally high cost-effectiveness and quality-of-life value.
- Chronic eczema is not merely a superficial skin disorder. It involves immune “memory” generated by bone marrow–derived immune cells. An organism long exposed to a Th2 cytokine-dominant environment requires sustained biochemical signaling to reset its inflammatory baseline. Seventy months of intervention spans multiple immune cell turnover cycles, potentially erasing 37 years of inflammatory imprinting at the cellular level.
Privacy
In situations where the disease information had already been made publicly available (as evidenced by prior articles), genuine names of individuals have been utilized. Conversely, in instances where there was no pre-existing public disclosure or at the explicit request of patients for privacy, pseudonyms have been employed. Furthermore, identities have been deliberately obscured, and certain contextual details and diagnoses have been modified to hinder any attempts at identification. It is essential to emphasize that the patients and encounters described in this work are authentic, and their consent for publication was duly obtained. As responsible authors, we earnestly implore all our readers to honor the privacy and confidentiality of these individuals. Additionally, certain scenarios, assessments, and clinical interventions have been altered to safeguard the anonymity of both patients and healthcare providers.
——————
这是一场跨越 70 个月(近 6 年)的皮肤修复实录。 本文记录了一位有着 37 年重度湿疹病史的女性患者,在摆脱长期激素依赖后,通过个体化草本系统调理实现“皮肤重生”的全过程的核心临床观察。我们不只是压制症状;我们是在用六年时间,重新编程那三十七年的炎症记忆:
- 康复非线性: 皮肤的修复并非一蹴而就,而是经历了从“炎症爆发(激素戒断期)”到“免疫纠偏”,再到“结构重塑”和“长期稳态”的四个关键阶段。
- 打破循环: 传统的“压制—反弹”模式无法根治慢性炎症。本案例证明,系统性的免疫调节(Systemic Regulation)可以重塑受损的皮肤屏障并平息过度活跃的免疫记忆。
- 时间成本与价值: 修复受损 30 余年的免疫系统需要与其病理深度相符的“生物时间”。在 70 个月的随访中,患者最终实现了无药维持的临床自愈,这为慢性特应性皮炎(AD)的长期管理提供了全新的科学实证。
病例背景
一名 37 岁女性患者,自婴儿期起即出现湿疹病史,累计病程 37 年。传统管理中长期使用外用类固醇,症状虽短期缓解,但停药后迅速复发,且每次复发更为严重。这种反复的炎症循环未能根本稳定免疫系统,反而加深了皮肤结构的慢性改变与瘙痒敏感性。患者未接受现代生物制剂治疗,而是在 Tangs Clinical TCM 接受了每月复诊、动态调整的个体化中药(植物药)治疗,连续跟踪 70 个月(约 6 年),通过阶段性照片记录与临床评估,观察皮肤状态的长期变化。
临床恢复的阶段性里程碑分析
在长达六年的治疗过程中,患者的皮肤表现经历了从“炎症活跃”到“结构修复”再到“稳态维持”的演变。这种缓慢而稳步的改善,是慢性湿疹重塑轨迹的真实写照:炎症缓解先于厚度恢复,而厚度与神经敏感性改善往往需要更长时间。
初始期(第0至9个月):炎症负荷的集中释放在停止使用所有类固醇后的最初几个月,患者表现出明显的红斑持续及苔藓样增厚,这属于典型的外用类固醇戒断反应 。皮肤炎症显著加重,红斑、瘙痒和皮肤敏感性上升,反映局部免疫调节失衡和免疫反跳。皮肤在这一时期表现得极为脆弱,临床管理的重点在于通过系统性调理缓解急性炎症波峰。
中期(第10至26个月):免疫失衡的逐步修正 进入第二年,红斑的活跃度开始显著降低,皮损的边界从模糊转为清晰。虽然皮肤厚度(苔藓样变)的改善相对缓慢,但急性发作的频率和强度已大幅下降 。这一过程验证了慢性湿疹的重塑轨迹:免疫信号的稳定往往先于物理结构的恢复。
后期(第28至46个月):表皮结构的实质性重塑在治疗的第三至第四年,观察到了表皮厚度的显著下降。通过肉眼及影像记录可以发现,原本粗糙、皮革样变的皮肤逐渐软化,红斑色调转为暗淡,这标志着角质层功能正在从分子层面进行修复。
稳定阶段(第48至70个月):长效稳态的建立在最后的两年里,患者皮肤趋于平整,无明显炎性红斑或渗出。残余的轻度色素沉着是长年炎症留下的唯一痕迹。此阶段的意义在于,患者无需依赖任何免疫抑制药物即可维持皮肤的自然健康状态,实现了真正的临床康复。
最大决定因素:反复类固醇使用历史
大量临床经验和学术报道均提示,反复使用外用类固醇不仅不能根治慢性湿疹,还可能导致所谓的“外用类固醇戒断症候群Topical Steroid Withdrawal (TSW),表现为停药后红斑、瘙痒加剧、皮肤敏感性上升等。长期的“压制—反弹—再压制”循环使得免疫状态与皮肤结构不断波动,从而加深了病理层面的慢性改变。文献指出,类固醇使用时间越长,恢复到稳态所需的时间越长,这在本病例中得到了直观验证。
系统性调理的科学依据
本病例中的治疗不是简单地“消炎”,而是通过辨证施治、个体化中药方剂系统性调理,逐步纠正免疫失衡和屏障功能异常,这与现代慢性病管理的概念高度一致:
- 系统层面调节免疫:中药复方中的活性成分已在实验研究中显示能调控炎症细胞因子(如 IL-4、IL-13)、促进 Th1/Th2 平衡、降低过敏反应强度;
- 促进屏障功能恢复:某些植物提取物可增强角质层中关键结构蛋白的表达(如 Filaggrin、Ceramide 合成途径),有助于修复皮肤天然屏障;
- 调整神经-免疫交互:慢性瘙痒的持续性部分源自神经敏感化;中药体系通过整体调理可缓冲这种敏感性,有助于减少抓挠行为并改善睡眠质量。
这些机制与当前针对慢性炎症的系统性管理趋势相通,与单一抑制炎症不同,它强调的是从免疫、屏障和神经三个维度推动整体稳态改善。
文献支持与科学基底
众多研究论证了免疫调节与屏障修复在慢性湿疹中的核心作用。例如:
- 现代病理生理学分析认为慢性湿疹不仅是局部炎症,还涉及免疫记忆和系统性炎症基线的重构;
- 综述性研究指出某些中草药成分具有炎症调节、抗氧化和屏障支持作用,被纳入多个传统医学体系用于慢性炎症状态;
- 慢性湿疹长期复发性特征的临床研究指出,仅仅抑制炎症信号并不能保证长期稳定,需从更高层次调节整体免疫稳态。
这些文献基础与本案例的长期追踪结果一致,均指向慢性病理的系统性调整需要更长的时间尺度,而非短期抑制即可解决。
临床与科学启示
- 长期管理 ≠ 愈合延迟
慢性湿疹的重建过程本质上是一个免疫-结构-神经系统稳态重建过程,其时间尺度应与病理深度相匹配。 - 类固醇历史为关键权重因子
长期反复使用外用类固醇是决定病情难治性与恢复时间延长的最大可变因素。 - 个体化中药调理具备系统性优势
相比只针对症状的抑制性策略,此类调理侧重免疫与屏障的整体重构,这与现代慢性病管理理念契合。
结论
在一个病程超过三十年的慢性湿疹临床案例中,采用个体化中药复方治疗伴随持续月度复诊的策略,最终实现了逐步的炎症控制、组织结构改善和长期稳定,这一轨迹反映了慢性炎症疾病自我稳态重建的真实过程。中医学与现代医学中追求的“精准医疗”相似,个体化中药调理强调的是根据患者的实时状态(辨证施治)动态调整药物配比,这在本质上是一种高度灵活的反馈系统 。
本案例强调
治疗时间的长短不是衡量疗效的唯一标准,而是与病理深度、历史治疗模式、免疫与屏障状态密切相关的生物学时间尺度。本报告对医疗行业提出的最大挑战在于对“疗效”定义的重审。如果以一个月为期限,该治疗方案可能被判定为“起效缓慢”;但如果以十年为期限,它所实现的无药稳态则具有极高的性价比和生命质量价值。慢性湿疹不仅仅是皮肤表面的问题,它涉及骨髓产生的免疫细胞的“记忆”。长期处于 Th2细胞因子优势环境下的机体,需要长时间的生化信号引导才能重置其炎症基线。70个月的干预时间,足以跨越多次免疫细胞的更新周期,从而在细胞层面抹去长达37年的炎症烙印。
Reference
- Atopic Dermatitis.Lancet. 2025. Guttman-Yassky E, Renert-Yuval Y, Brunner PM.
- Atopic Dermatitis (Eczema) Guidelines: 2023 American Academy of Allergy, Asthma and Immunology/American College of Allergy, Asthma and Immunology Joint Task Force on Practice Parameters GRADE- And Institute of Medicine-Based Recommendations.
- Annals of Allergy, Asthma & Immunology : Official Publication of the American College of Allergy, Asthma, & Immunology. 2024. Chu DK, Schneider L, Asiniwasis RN, et al.Guideline
- Strategies for Using Topical Corticosteroids in Children and Adults With Eczema. The Cochrane Database of Systematic Reviews. 2022. Lax SJ, Harvey J, Axon E, et al.
- Guidelines of Care for the Management of Atopic Dermatitis in Adults With Topical Therapies. Journal of the American Academy of Dermatology. 2023. Sidbury R, Alikhan A, Bercovitch L, et al.
- Progression of Acute-to-Chronic Atopic Dermatitis Is Associated With Quantitative Rather Than Qualitative Changes in Cytokine Responses. The Journal of Allergy and Clinical Immunology. 2020. Tsoi LC, Rodriguez E, Stölzl D, et al.
- Atopic Dermatitis Displays Stable and Dynamic Skin Transcriptome Signatures. The Journal of Allergy and Clinical Immunology. 2021.
- A Mild Topical Steroid Leads to Progressive Anti-Inflammatory Effects in the Skin of Patients With Moderate-to-Severe Atopic Dermatitis. The Journal of Allergy and Clinical Immunology. 2016.
- Examining the Unanswered Questions in TSW: A Case Series of 16 Patients and Review of the Literature.Journal of Clinical Medicine. 2026. Lu MY, Erickson A, Vijendra A, et al.
- A Systematic Review of Topical Corticosteroid Withdrawal (“Steroid Addiction”) in Patients With Atopic Dermatitis and Other Dermatoses.Journal of the American Academy of Dermatology. 2015. Hajar T, Leshem YA, Hanifin JM, et al.
- Topical Steroid Withdrawal: A Case Series of 10 Children. Acta Dermato-Venereologica. 2019. Sheary B.
- Rebounding Triad (Severe Itching, Dryness and Burning) After Facial Corticosteroid Discontinuation Defines a Specific Class of Corticosteroid-Dependent Dermatitis.The Journal of Dermatology. 2015. Xiao X, Xie H, Jian D, et al.
- Modulation of Epidermal Terminal Differentiation in Patients After Long-Term Topical Corticosteroids. The Journal of Dermatology. 1991. Sheu HM, Tai CL, Kuo KW, Yu HS, Chai CY.
- Alterations in Water Content of the Stratum Corneum Following Long-Term Topical Corticosteroids. Journal of the Formosan Medical Association = Taiwan Yi Zhi. 1991. Sheu HM, Chang CH.
- Morphologic Investigations on the Rebound Phenomenon After Corticosteroid-Induced Atrophy in Human Skin. The Journal of Investigative Dermatology. 1984. Zheng PS, Lavker RM, Lehmann P, Kligman AM.
- Corticosteroid Exposure and Cumulative Effects in Patients With Eczema: Results From a Patient Survey. Annals of Allergy, Asthma & Immunology : Official Publication of the American College of Allergy, Asthma, & Immunology. 2023. Barta K, Fonacier LS, Hart M, et al.
- Values and Preferences of Patients and Caregivers Regarding Treatment of Atopic Dermatitis (Eczema): A Systematic Review. JAMA Dermatology. 2023. Maleki-Yazdi KA, Heen AF, Zhao IX, et al.
- Efficacy and Action Mechanisms of a Chinese Herbal Formula on Experimental Models of Atopic Dermatitis. Journal of Ethnopharmacology. 2021. Wang L, Xian YF, Hu Z, et al.
- Anti-Inflammatory Effects of the LK5 Herbal Complex on LPS- And IL-4/IL-13-Stimulated HaCaT Cells and a DNCB-Induced Animal Model of Atopic Dermatitis in BALB/c Mice. Pharmaceutics. 2023. Kim HJ, Kim SY, Bae HJ, et al.
- Natural Products Modulating Interleukin-Mediated Pathways for Anti-Allergic and Immunomodulatory Effects. Natural Product Reports. 2026. Shah AB, Kim YJ, Lee KS, et al.
- The Influence of Traditional Herbal Formulas on Cytokine Activity. Toxicology. 2010. Burns JJ, Zhao L, Taylor EW, Spelman K.
- Chinese Herbal Medicine and Their Active Ingredients Involved in the Treatment of Atopic Dermatitis Related Signaling Pathways. Phytotherapy Research : PTR. 2025. Nie W, Fu H, Zhang Y, Yang H, Liu B.
- Traditional Chinese Medicine for Food Allergy and Eczema. Annals of Allergy, Asthma & Immunology : Official Publication of the American College of Allergy, Asthma, & Immunology. 2021. Wang Z, Wang ZZ, Geliebter J, Tiwari R, Li XM.
- Phytotherapeutic Potential of Natural Herbal Medicines for the Treatment of Mild-to-Severe Atopic Dermatitis: A Review of Human Clinical Studies. Biomedicine & Pharmacotherapy = Biomedecine & Pharmacotherapie. 2017. Hussain Z, Thu HE, Shuid AN, et al.
- Effectiveness and Safety of Herbal Medicine for Atopic Dermatitis: An Overview of Systematic Reviews. Evidence-Based Complementary and Alternative Medicine : eCAM. 2020. Kwon CY, Lee B, Kim S, et al.
- Atopic Dermatitis-Related Anti-Inflammatory in Vitro Effects of a Plant Extract Mixture. Scientific Reports. 2025. Heinemann N, Rademacher F, Vollert H, Gläser R, Harder J.
- Regulatory Effects of Ishige Okamurae Extract and Diphlorethohydroxycarmalol on Skin Barrier Function. Heliyon. 2024. Bak SG, Lim HJ, Won YS, et al.
- Eucalyptus Increases Ceramide Levels in Keratinocytes and Improves Stratum Corneum Function. International Journal of Cosmetic Science. 2012. Ishikawa J, Shimotoyodome Y, Chen S, et al.
- Echinacea Purpurea-Derived Alkylamides Exhibit Potent Anti-Inflammatory Effects and Alleviate Clinical Symptoms of Atopic Eczema. Journal of Dermatological Science. 2017. Oláh A, Szabó-Papp J, Soeberdt M, et al.
- Efficacy and Safety of Chinese Herbal Medicine in the Treatment of Chronic Pruritus: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Frontiers in Pharmacology. 2023. Wang J, Chen Y, Yang X, et al.
- Mast Cell-Neuron Axis as a Core Mechanism in Chronic Pruritus of Atopic Dermatitis: From Mechanistic Insights to Therapeutic Targets.
Frontiers in Immunology. 2025. Li D, Han Y, Zhou J, et al. - A Topical Chinese Herbal Inhibits Pruritus and Skin Inflammation via Neural TRPM8 in Atopic Dermatitis. Phytomedicine : International Journal of Phytotherapy and Phytopharmacology. 2025. Chen Y, Tang Z, Han Z, et al
- Neuroimmune Communication Regulating Pruritus in Atopic Dermatitis. The Journal of Allergy and Clinical Immunology. 2022. Steinhoff M, Ahmad F, Pandey A, et al.
- Neuronal Regulation of Inflammation in Atopic Dermatitis. International Archives of Allergy and Immunology. 2025. Zhang CY, Jin YM, Liu RF, Wang Y.
- Pathogenic Mechanisms Underlying Itch in Atopic Dermatitis: The Emerging Role of Neuroimmune Interactions. European Journal of Dermatology : EJD. 2023. Escalante A, Serra-Baldrich E.
- Alterations in Brain Neural Network and Stress System in Atopic Dermatitis: Novel Therapeutic Interventions. The Journal of Pharmacology and Experimental Therapeutics. 2023. Nakagawa Y, Yamada S.
- Progression of Acute-to-Chronic Atopic Dermatitis Is Associated With Quantitative Rather Than Qualitative Changes in Cytokine Responses. The Journal of Allergy and Clinical Immunology. 2020. Tsoi LC, Rodriguez E, Stölzl D, et al.
- The Immunology of Atopic Dermatitis and Its Reversibility With Broad-Spectrum and Targeted Therapies. The Journal of Allergy and Clinical Immunology. 2017. Brunner PM, Guttman-Yassky E, Leung DY.
- Epigenetic Control of Inflammation in Atopic Dermatitis. Seminars in Cell & Developmental Biology. 2024. Akhtar S, Alsayed RKME, Ahmad F, et al
- Harnessing Antioxidant Properties of Plant-Derived Bioactive Compounds to Alleviate Atopic Dermatitis Symptoms: A Review. Current Pharmaceutical Design. 2025. Chandimali N, Hong SM, Bae J, et al.
- Research Progress on Traditional Chinese Medicine Compounds in Autoimmune-Related Skin Diseases. Frontiers in Immunology. 2025. Wang Y, Bu P, Deng Y, Zhao W, Pan G.
- Flavonoids as Natural Anti-Inflammatory Agents in the Atopic Dermatitis Treatment.Pharmaceutics. 2025. Zawawi NA, Ahmad H, Madatheri R, et al.
- Phytomedicines Are Efficient Complementary Therapies for the Treatment of Atopic Dermatitis: A Review of Mechanistic Insight and Recent Updates. Current Drug Targets. 2017. Tumpang MA, Ramli NA, Hussain Z.
- Atopic Dermatitis-Related Anti-Inflammatory in Vitro Effects of a Plant Extract Mixture. Scientific Reports. 2025. Heinemann N, Rademacher F, Vollert H, Gläser R, Harder J.
- Long-Term Progressive Improvement of Atopic Dermatitis by an Herbal Emollient Plus Combination in a 12-Week Clinical Trial. Acta Dermato-Venereologica. 2025. Herrmann L, Andreev S, Ziegler R, et al.
- Topical Chinese Herbal Medicine in Treating Atopic Dermatitis (Eczema): A Systematic Review and Meta-Analysis With Core Herbs Exploration. Journal of Ethnopharmacology. 2023. Wang MC, Chou YT, Kao MC, et al.
- Management of Atopic Dermatitis via Oral and Topical Administration of Herbs in Murine Model: A Systematic Review. Frontiers in Pharmacology. 2021. Mohd Kasim VNK, Noble SM, Liew KY, et al.
- Phytotherapeutic Potential of Natural Herbal Medicines for the Treatment of Mild-to-Severe Atopic Dermatitis: A Review of Human Clinical Studies. Biomedicine & Pharmacotherapy = Biomedecine & Pharmacotherapie. 2017. Hussain Z, Thu HE, Shuid AN, et al.
- Chinese Herbal Medicine for Atopic Eczema. The Cochrane Database of Systematic Reviews. 2013. Gu S, Yang AW, Xue CC, et al.
- Subclinical Inflammation Precedes Atopic Dermatitis Relapses. The Journal of Allergy and Clinical Immunology. 2025. Al B, Holzscheck N, Traidl S, et al.
- Progression of Acute-to-Chronic Atopic Dermatitis Is Associated With Quantitative Rather Than Qualitative Changes in Cytokine Responses. The Journal of Allergy and Clinical Immunology. 2020. Tsoi LC, Rodriguez E, Stölzl D, et al.
- Are the Concepts of Induction of Remission and Treatment of Subclinical Inflammation in Atopic Dermatitis Clinically Useful? The Journal of Allergy and Clinical Immunology. 2014. Tang TS, Bieber T, Williams HC.
- Role of Skin-Homing T-Cells in Recurrent Episodes of Atopic Dermatitis: A Review. Frontiers in Immunology. 2024. Guo H, Yuan H, Yu Y, et al.
- Integrated Clinical Trial and Molecular Profiling Reveals Immune Drivers of Chronic Hand Eczema.
Allergy. 2026. Gery P, Ekren R, Bérard E, et al.



