Steroids Rosacea Overlaps Retinoid Dermatitis 激素性皮炎叠加维A酸皮炎
A 54-year-old woman presented with 3 months of facial rash. The rash persisted despite a recent 2-month applicaiton of various corticosteroids daily, prescribed for eczema. The patient reported a 2-week history of acne treated by retinoid cream when she entered menopause 6 months before the current presentation. She also had a 10-year history of hypertension.
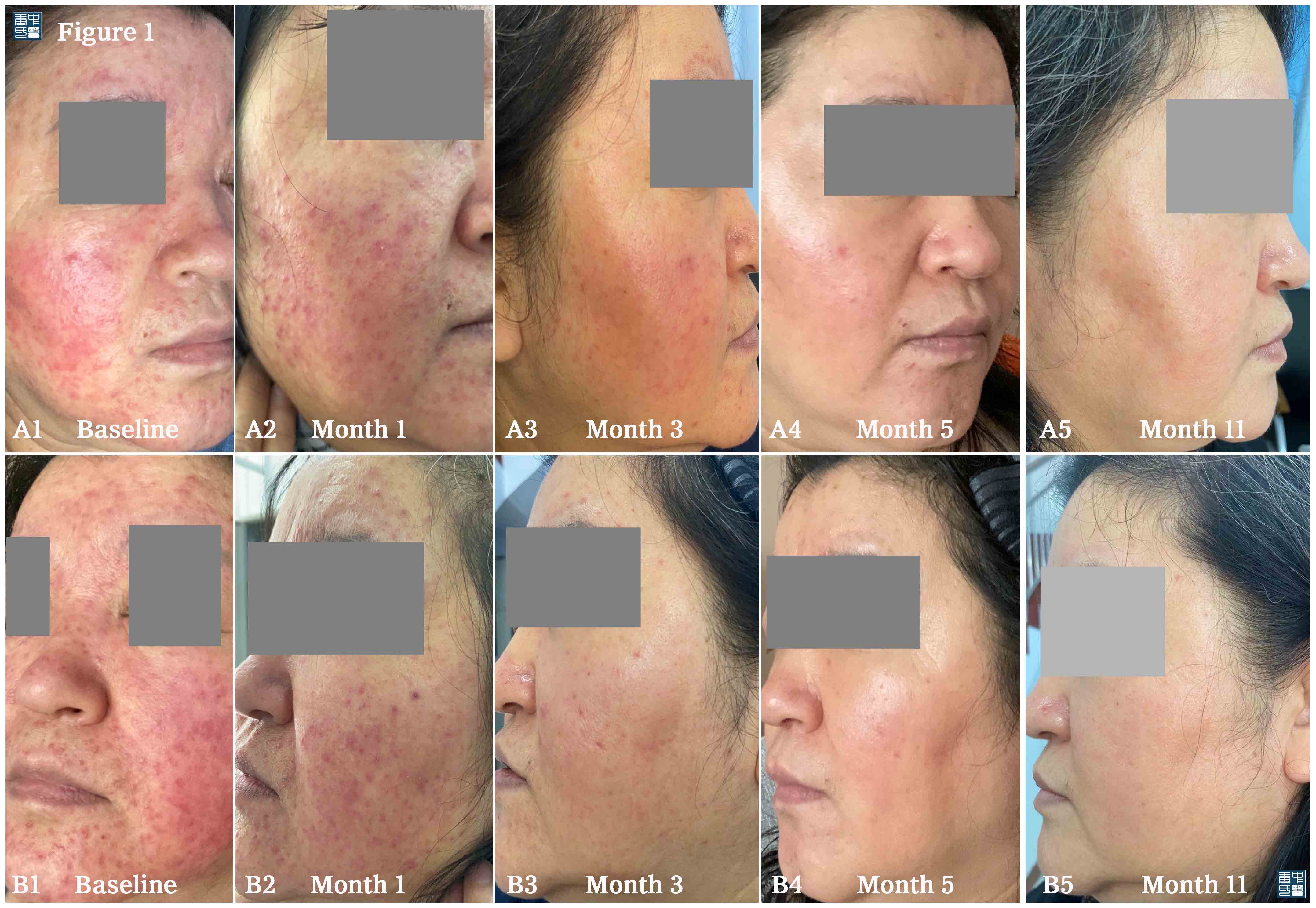
Physical examination revealed numerous red papules and pustulation formed on the cheeks (Fig.A1, B1).
Patient History
Some women experience acne during menopause. This is likely due to a drop in estrogen levels or an increase in androgen hormones like testosterone. Acne in perimenopausal women is rarely severe enough to warrant medical treatment, and once your hormones balance out, the acne usually disappears. The patient applied the topical retinoid clearing the menopause acne, however, topical therapy with retinoids result in unwanted cutaneous dermatitis, including erythema and scaling [1-2] which is called retinoid dermatits. The retinoid dermatitis is associated to the type and dose of the retinoid and typically occurs within 2–4 days of initial treatment [2], it may be mistaken for eczema. Her physician prescribed topical steroids to suppress the “eczema”, which initially gave pleasing results, but tolerance occured. New potent topical steroid was administrated to suppress the erythema and pustules that reappeared following the use of the weaker steroid. Hence steroids rosacea, also known as steroids withdrawal syndrome, developed (Fig.A1, B1).
Discussion and Treatment
The patient with facial rashes displays the characteristics of rosacea, retinoid dermatitis, steroids induced dermatitis, eczema, seborrheic dermatitis, dermatomyositis, or systemic lupus erythematosus (SLE). These conditions can be mistaken for one another, but obtaining a patient history and conducting a careful examination of the morphologic features of the rash can allow for determination of the likely cause. On the basis of the symptoms and the morphologic features of facial rash in this woman, steroids rosacea (dermatitis) overlaps retinoid dermatitis is the most likely diagnosis.
We advise her to cease the usage of steroid cream, and the regimen of herbal medicine daily was started, and there was substantial improvement in the cutaneous findings. The patient had a complete response to herbal medication, with the 5th month’s examination revealing full clearance of facial rash.
Epilogue
The most recent feedback updated from the patient on 18 March 2021.


Reference:
- Griffiths CE, Finkel LJ, Tranfaglia MG, et al: An in vivo experimental model for effects of topical retinoic acid in human skin. Br J Dermatol 1993; 129: pp. 389-394
- Griffiths CE, Kang S, Ellis CN, et al: Two concentrations of topical tretinoin (retinoic acid) cause similar improvement of photoaging but different degrees of irritation. A double-blind, vehicle-controlled comparison of 0.1% and 0.025% tretinoin creams. Arch Dermatol 1995; 131: pp. 1037-1044



